An International Standard for Resuscitative Hemostasis : Massive Transfusion Protocol (MTP)
In the high-stakes environment of general surgery, uncontrolled hemorrhage remains a leading cause of preventable mortality. Whether from traumatic injury, catastrophic gastrointestinal bleeding, or a major surgical complication, the rapid loss of blood leads to a lethal triad of acidosis, hypothermia, and coagulopathy. To combat this, the medical community has developed and standardized a critical response system: the Massive Transfusion Protocol (MTP).
An MTP is a pre-established, structured set of procedures activated to deliver large volumes of blood products rapidly and systematically to a patient experiencing massive hemorrhage. It transcends a simple large order of blood; it is a coordinated, multidisciplinary effort involving surgery, anesthesiology, nursing, and the blood bank, designed to restore circulation, correct coagulopathy, and save lives.
Defining the Crisis: Diagnosis and Activation Criteria
The decision to activate an MTP is clinical and should not be delayed for laboratory results. Speed is paramount. Internationally accepted criteria for MTP activation include:
- Clinical Assessment: Obvious uncontrolled bleeding in the OR or ED, or a patient in profound hemorrhagic shock unresponsive to initial fluid resuscitation.
- Blood Loss Volume: Acute blood loss exceeding 50% of total blood volume within 3 hours, or a rate of loss of 150 mL/min.
- Physiological Parameters: Systolic blood pressure < 90 mmHg and heart rate > 120 bpm, with signs of poor perfusion.
- Point-of-Care Testing (POCT): The use of viscoelastic hemostatic assays (VHA) like TEG (Thromboelastography) or ROTEM (Rotational Thromboelastometry) is increasingly used to provide a rapid, real-time assessment of clot formation and guide MTP activation and management.
The Cornerstone of Modern Resuscitation: Balanced Transfusion
The historical approach of crystalloid and packed red blood cell (PRBC) infusion alone often worsened coagulopathy by diluting clotting factors and platelets. The modern, internationally accepted principle of MTP is balanced resuscitation or hemostatic resuscitation. This means transfusing blood products in a ratio that approximates whole blood, proactively preventing and treating coagulopathy.
The most widely endorsed and evidence-based ratio is the 1:1:1 ratio, which for every 1 unit of PRBCs, provides 1 unit of Fresh Frozen Plasma (FFP), and 1 unit of platelets (often as a single donor apheresis unit).
- Packed Red Blood Cells (PRBCs): Restore oxygen-carrying capacity and intravascular volume.
- Fresh Frozen Plasma (FFP): Provides essential clotting factors (II, V, VII, VIII, IX, X, XIII) and fibrinogen to support clot formation.
- Platelets: Critical for primary hemostasis and forming the initial platelet plug.
- Cryoprecipitate or Fibrinogen Concentrate: Often incorporated as a fourth component, especially when fibrinogen levels are critically low (<1.5 g/L). Cryoprecipitate is a rich source of fibrinogen, Factor VIII, and von Willebrand factor.
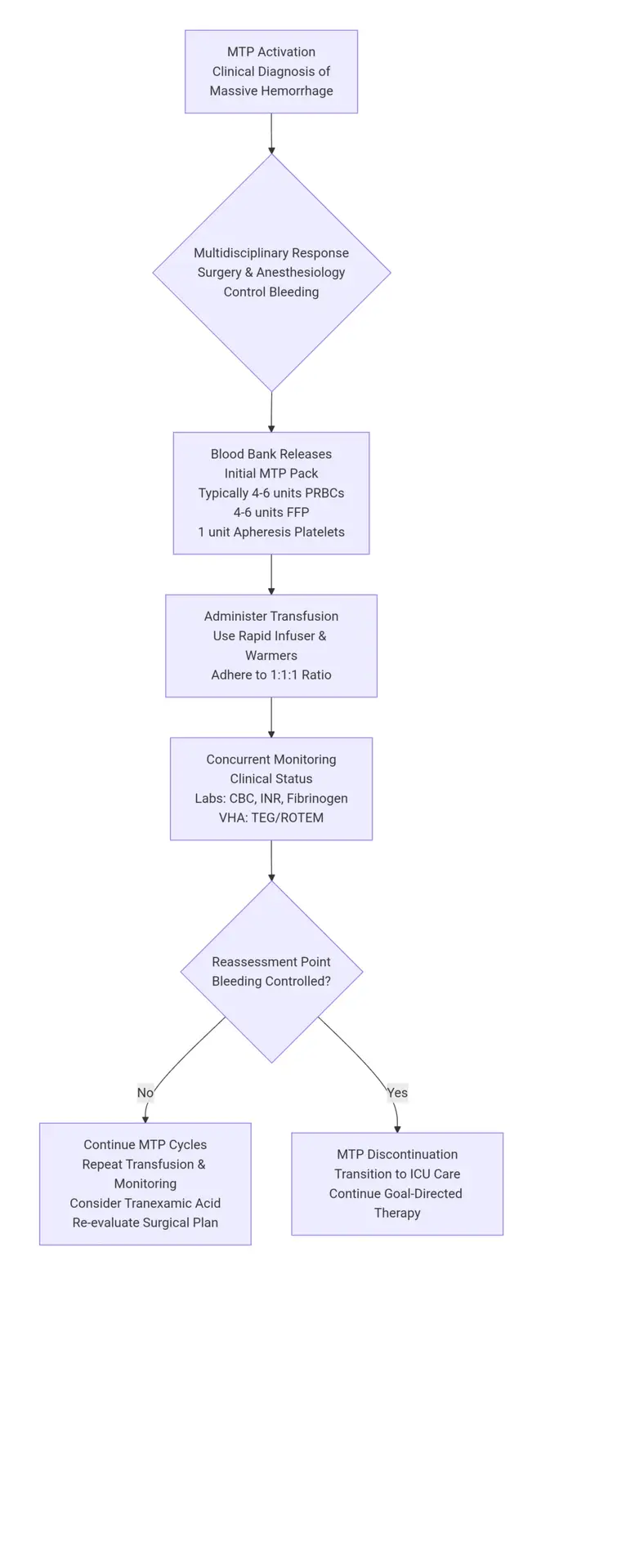
The MTP in Action: A Standardized Flowchart
The following flowchart illustrates a typical, internationally recognized MTP sequence. It is a cyclical process of administer-monitor-reassess.
Ethical Values in MTP Implementation
The deployment of an MTP is not just a technical procedure; it is guided by core ethical principles:
- Beneficence and Non-maleficence: The primary goal is to do good by saving a life. However, this is balanced against the duty to avoid harm. MTPs carry risks, including transfusion-related acute lung injury (TRALI), circulatory overload (TACO), and immunologic reactions. The protocol must be managed to maximize benefit and minimize these risks.
- Justice and Resource Stewardship: Blood products are a finite, community-sourced resource. Activating an MTP for a patient with a high chance of survival is a just use. However, futile resuscitation in unsalvageable patients (e.g., non-survivable injuries) raises ethical concerns about resource allocation and distributive justice. Clear institutional guidelines for MTP initiation and termination are essential.
- Patient Autonomy and Consent: In an emergency, MTP is initiated under the principle of implied consent for life-saving treatment. However, if a patient has a known advance directive (e.g., a Jehovah’s Witness with specific blood product refusal), these wishes must be respected to the greatest extent possible, and alternative strategies (hemostatic agents, volume expanders) must be employed.
Adjuncts to MTP: The Comprehensive Treatment Plan
A successful MTP is part of a broader damage control philosophy.
- Damage Control Surgery (DCS): The focus shifts from definitive repair to rapid control of bleeding and contamination. The procedure is abbreviated, and the patient is transferred to the ICU for resuscitation and rewarming before returning for definitive surgery.
- Pharmacological Agents:
- Tranexamic Acid (TXA): An antifibrinolytic agent that inhibits clot breakdown. International guidelines (e.g., CRASH-2 trial) recommend its administration within 3 hours of injury in trauma settings.
- Calcium: Citrate in blood products binds calcium, leading to hypocalcemia that impairs cardiac function and clotting. Ionized calcium levels must be monitored and supplemented.
- Prothrombin Complex Concentrates (PCC): Used in specific situations, such as reversal of vitamin K antagonists.
- Goal-Directed Therapy: As the patient stabilizes, resuscitation transitions from fixed-ratio to goal-directed therapy, guided by frequent lab tests and VHA, to tailor product administration and avoid complications of over-transfusion.
The Massive Transfusion Protocol represents a paradigm shift in the management of life-threatening hemorrhage. By standardizing a multidisciplinary response around the principle of balanced hemostatic resuscitation, it has significantly improved patient outcomes globally. Its successful implementation hinges not only on a clear, efficient institutional protocol but also on a deep understanding of the underlying diagnosis, the adjunctive treatments, and the profound ethical responsibilities involved in administering one of the most resource-intensive interventions in modern medicine. For the general surgeon, proficiency in activating and managing an MTP is an indispensable skill in the relentless pursuit of saving lives.