Preparing for Surgery: Understanding the Critical Role of Fasting (NPO)
Before any scheduled surgical procedure, a universal instruction given to patients is to refrain from eating or drinking. This medical directive, known as NPO (from the Latin nil per os, meaning “nothing by mouth”) or preoperative fasting, is far more than a simple guideline, it is a fundamental safety protocol essential for preventing one of the most serious risks in anesthesia: pulmonary aspiration.
Aspiration occurs when stomach contents are inadvertently inhaled into the lungs. Under anesthesia, the body’s natural protective reflexes, such as coughing and gagging, are suppressed. If the stomach contains food or acidic fluids, even a small amount entering the airway can cause significant damage, leading to a life-threatening condition known as aspiration pneumonitis.
This introduction explores the vital principles behind NPO guidelines, explaining why this period of metabolic rest is a cornerstone of patient safety in modern general surgery. We will demystify the standard “nothing after midnight” rule, clarify the updated distinctions between clear liquids and solid foods, and highlight how this crucial preparation contributes to a safer surgical outcome for every patient.
Preoperative Fasting Guidelines – Surgical Patient Safety Protocol
- Preoperative fasting is a crucial patient safety measure aimed at reducing the risk of aspiration during anesthesia.
- Modern guidelines focus on balancing patient safety and comfort by allowing appropriate intake of clear fluids and carbohydrates before surgery.
- These recommendations are based on standards from the American Society of Anesthesiologists (ASA), European Society of Anaesthesiology (ESA), and ERAS® (Enhanced Recovery After Surgery) protocols.
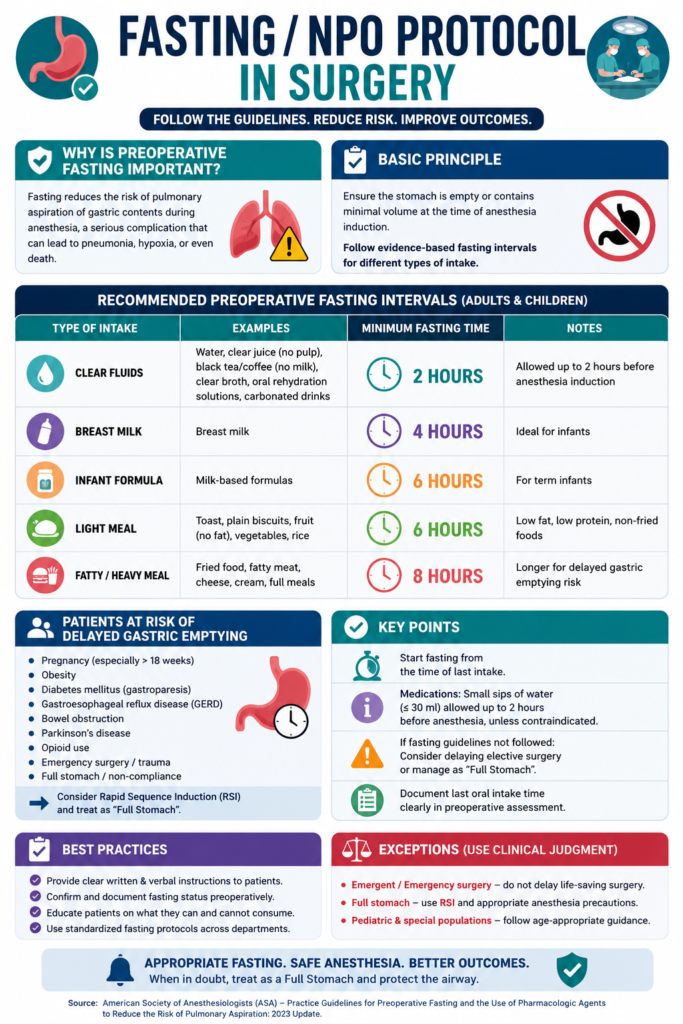
Fasting Duration Recommendations
Evidence-based fasting intervals before anesthesia:
- Clear Liquids:
- Fast for 2 hours before surgery.
- Includes water, clear juice, tea, or black coffee.
- Encouraged up to 2 hours before induction for hydration and comfort.
- Breast Milk:
- Fast for 4 hours (infants only).
- Allows partial gastric emptying with moderate digestion time.
- Infant Formula:
- Fast for 6 hours (for non-breastfed infants).
- Slower gastric emptying than breast milk.
- Light Meal:
- Fast for 6 hours.
- Includes toast, crackers, or soup with low fat content.
- Regular Meal:
- Fast for 8 hours or more.
- Avoid fatty, fried, or heavy meals due to delayed gastric emptying.
Stepwise Fasting Protocol
- Patient Assessment
- Evaluate gastrointestinal function and comorbidities.
- Identify conditions causing delayed gastric emptying (e.g., GERD, diabetes, obesity, pregnancy).
- Document risk factors for aspiration.
- Individualized Planning
- Tailor fasting durations based on patient risk profile.
- High-risk patients (e.g., GERD, obesity) may need extended fasting (8+ hours).
- Use minimal fasting for low-risk patients to prevent dehydration or hypoglycemia.
- Preoperative Carbohydrate Loading
- Give clear carbohydrate drinks 2–3 hours before surgery (for suitable patients).
- Benefits include reduced thirst and hunger, improved insulin sensitivity, and decreased metabolic stress.
- Avoid in cases of delayed gastric emptying or gastroparesis.
- Medication Management
- Continue essential medications (e.g., cardiac, anticonvulsant, or psychiatric drugs) with small sips of water.
- Adjust or withhold diuretics, oral hypoglycemics, and insulin as per anesthesia team advice.
Special Considerations
- Pediatric Patients
- Clear fluids: 2 hrs | Breast milk: 4 hrs | Formula: 6 hrs | Solids: 8 hrs.
- Schedule morning procedures to reduce fasting stress.
- Diabetic Patients
- Prioritize morning slots.
- Use individualized insulin and glucose control plans.
- Monitor blood glucose closely during fasting period.
- Pregnant Patients
- Considered high aspiration risk.
- Use antacids, left uterine displacement, and rapid sequence induction.
- Emergency Surgery
- Assume full stomach.
- Use rapid sequence induction, apply cricoid pressure, and ensure suction readiness.
Evidence and Outcomes
- Aspiration Risk:
- Occurs in 1 out of 3,000–5,000 cases; mortality around 1 in 65,000.
- Proper fasting significantly reduces gastric volume and acidity.
- Metabolic and Clinical Benefits:
- Maintains glycogen stores and improves postoperative glucose control.
- Reduces insulin resistance by up to 50%.
- Enhances patient comfort and satisfaction.
- ERAS Outcomes:
- Reduces hospital stay by 1–2 days.
- Decreases postoperative complications and improves recovery without increasing aspiration risk.
Implementation Notes
- Adapt protocols to each institution’s policies and surgical type.
- Use clinical judgment to modify fasting duration when needed.
- Educate patients on safe fasting practices and expected timelines.
- Ensure clear communication among surgical, anesthesia, and nursing teams.
- Regularly audit adherence to fasting protocols to ensure consistency and safety.