
What is Damage Control Surgery and Resuscitation? A Life-Saving Strategy in Trauma Care
In the high-stakes realm of trauma surgery, where patients hover on the brink of death, a conventional approach of meticulously repairing all injuries in one operation can be fatal. This is where the paradigm of Damage Control Surgery (DCS) and Damage Control Resuscitation (DCR) comes into play, a coordinated, life-saving strategy that prioritizes survival over completeness.
Think of it as a strategic retreat in a medical battle. Instead of fighting until every problem is solved, the team addresses only the immediate, life-threatening issues, like uncontrolled bleeding and massive contamination and then swiftly moves the patient to the ICU for stabilization. The core principle is simple but profound: A living patient with unfinished surgery is better than a dead patient with a technically perfect operation.
This approach is a two-phase process:
Damage Control Surgery (The Operation):
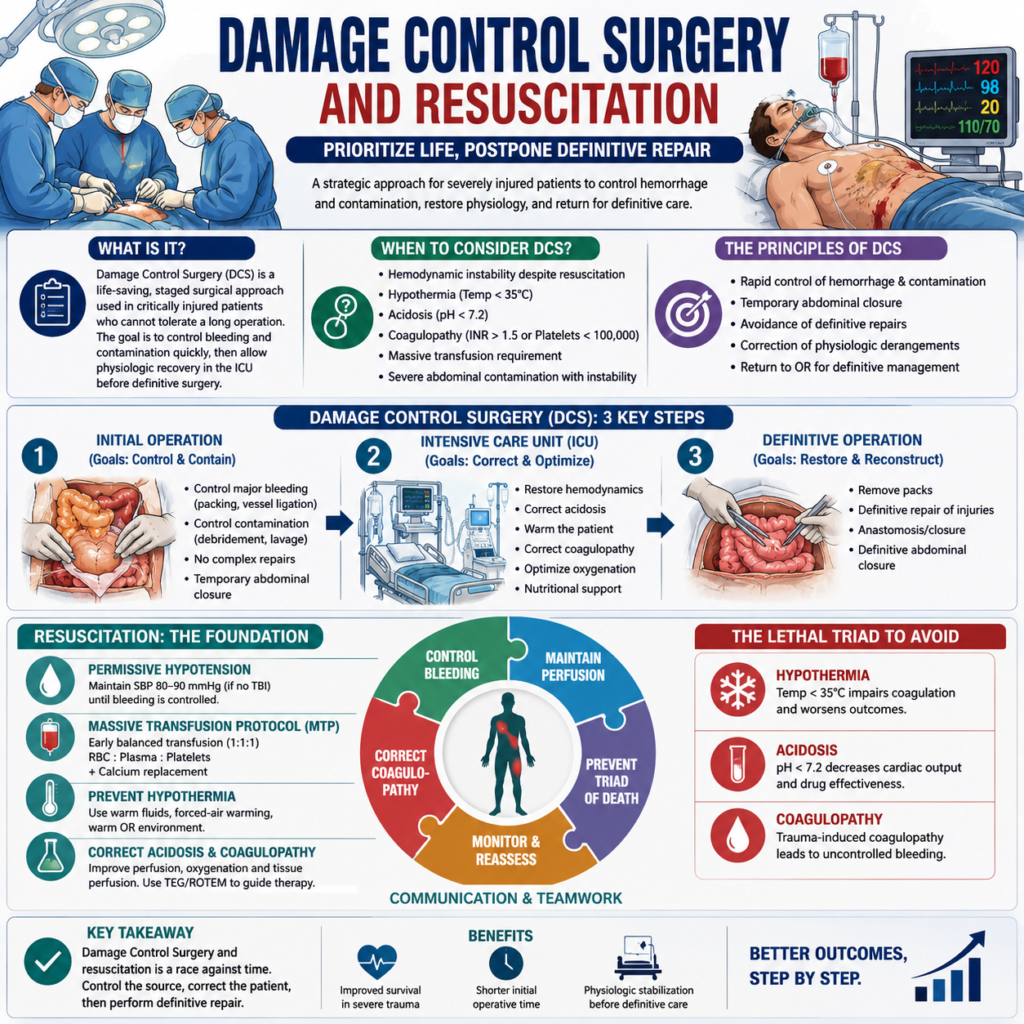
This initial phase is brutally efficient, typically lasting less than 90 minutes. The surgeon’s goal is not to fix everything but to “control damage” through three critical steps, control bleeding, control contamination from the gut, and leave the abdomen temporarily open to prevent abdominal compartment syndrome.
Damage Control Resuscitation (The ICU Care):
Simultaneously and following surgery, the patient undergoes aggressive physiological stabilization in the Intensive Care Unit. This involves correcting the “lethal triad” of trauma, hypothermia (low body temperature), acidosis (buildup of acid in the blood), and coagulopathy (inability to clot blood), using warmed fluids, blood product transfusions, and advanced monitoring.
Only once the patient’s physiology is normalized days later do they return to the operating room for definitive repair of all injuries. Damage Control is not a specific procedure but a overarching philosophy that has revolutionized modern trauma care, turning previously unsurvivable injuries into stories of survival.
Damage Control Surgery (DCS) is a life-saving surgical strategy designed to stabilize critically injured patients suffering from severe trauma. It focuses on rapid control of bleeding and contamination, followed by temporary closure and intensive care resuscitation before final repair. This staged approach is essential in managing patients who cannot tolerate prolonged definitive operations due to physiological instability.
Historical Evolution of Damage Control Surgery
In the early 20th century, surgeons attempted definitive repair for all injuries during the initial surgery, often leading to fatal outcomes. Over time, the “damage control” concept emerged, prioritizing patient survival over complete anatomical correction. The term gained popularity in the 1990s with advancements in trauma surgery and resuscitation science.
Goals and Principles of Damage Control Surgery
The primary goal of DCS is to save life by preventing the lethal triad of hypothermia, acidosis, and coagulopathy. Instead of performing complex reconstructive procedures immediately, surgeons aim to control bleeding, limit contamination, and restore physiological stability before completing definitive surgery.
Indications for Damage Control Surgery
DCS is indicated when patients present with:
Uncontrolled hemorrhage unresponsive to standard surgical control
Severe hypothermia (core temperature < 34°C)
Coagulopathy and metabolic acidosis
Multiple visceral injuries with hemodynamic collapse
Such patients cannot withstand a prolonged definitive operation and require a phased resuscitative approach.
Phases of Damage Control Surgery
Phase 1. Initial Operation (Control Phase)
This phase focuses on rapid hemorrhage and contamination control. The aim is not perfect repair but temporary stabilization to prevent further physiological decline.
Phase 2. Critical Care Resuscitation
After the initial operation, the patient is transferred to the ICU for intensive monitoring. Fluid balance, temperature, and coagulation are restored during this critical phase.
Phase 3. Definitive Reconstruction
Once the patient’s physiology stabilizes, definitive repair is carried out, involving organ reconstruction and closure of temporary surgical openings.
Step-by-Step Flowchart of Damage Control Surgery
- Assessment and Triage
Rapid trauma evaluation and prioritization
Identification of life-threatening injuries
- Rapid Hemorrhage Control
Temporary vascular control using packing or clamping
Avoiding time-consuming vascular anastomoses
- Containment of Contamination
Closure or isolation of perforated viscera
Temporary bowel diversion if necessary
- Temporary Closure and Transfer
Use of sterile temporary dressings or VAC systems
Immediate transfer to ICU for stabilization
- ICU Resuscitation and Monitoring
Correction of acidosis, hypothermia, and coagulopathy
Continuous monitoring of hemodynamics
- Definitive Surgery and Recovery
Final repair of organs and closure of abdominal cavity
Gradual transition to postoperative rehabilitation
Physiological Rationale Behind Damage Control Surgery
DCS is founded on the understanding of the lethal triad:
Hypothermia: Reduces clotting efficiency
Acidosis: Impairs cardiac and cellular function
Coagulopathy: Leads to uncontrolled bleeding
These factors form a vicious cycle that rapidly worsens patient outcomes if not interrupted through damage control measures.
Key Components in DCS Flowchart
A professionally educational flowchart for DCS should include:
- Clear depiction of each surgical phase
- Sequential steps from assessment to reconstruction
- Integration of decision points for surgical intervention
- Visual emphasis on resuscitation and ICU management
Role of Multidisciplinary Team in DCS
The success of DCS depends on seamless teamwork between trauma surgeons, anesthesiologists, and critical care specialists. Communication and real-time decision-making are critical for improving survival rates.
Challenges and Limitations
Despite its benefits, DCS faces challenges such as:
- Difficulty in managing temporary closures
- Risk of infection or abdominal compartment syndrome
- Delayed healing and complications from staged operations
- Proper postoperative care and vigilant monitoring are essential to mitigate these risks.
Benefits of Damage Control Surgery
- Enhanced survival in patients with severe trauma
- Reduced intraoperative mortality by limiting surgical time
- Better physiological recovery before definitive reconstruction
This approach allows surgeons to focus on saving life first, and structure later.
Innovations in Damage Control Surgery
Modern advancements such as vacuum-assisted closures, hemostatic sealants, and point-of-care monitoring have revolutionized DCS outcomes. Additionally, 3D imaging and AI-assisted triage enhance precision in trauma decision-making.
Damage Control Surgery
It represents a life-preserving evolution in trauma care, balancing urgency with precision. By understanding its stages and physiological rationale, both medical professionals and educators can enhance their practice and teaching. A well-structured SEO-optimized flowchart not only educates effectively but also strengthens the online visibility of surgical content.
FAQs
- What is the main goal of Damage Control Surgery?
To rapidly control bleeding and contamination, stabilize the patient, and perform definitive repair once physiology normalizes. - How does DCS differ from traditional surgery?
Traditional surgery seeks complete repair immediately, while DCS focuses on staged operations prioritizing survival first. - What are the three phases of DCS?
Initial control operation, intensive care resuscitation, and definitive reconstruction. - Why is the lethal triad important in DCS?
It guides the urgency of intervention to prevent hypothermia, acidosis, and coagulopathy-related deaths. - How can DCS be visually explained for educational purposes?
Through a clear flowchart detailing each stage—assessment, control, stabilization, and repair.